DALL-E, a text to image AI model, was opened to the general public in 2022. The result was a tsunami of additional image generators, to the point that the total number of AI images being created is estimated to be 34 million images every day. Even people who are not especially interested in art have probably seen some of the now classic AI art images, such as scenes of space fantasy, dystopian worlds, super heroes, surreal compositions and idealized models, usually female.
This is all missing some really wonderful uses for AI generated images.
After many years reading about science, I realized that I didn’t have a good idea of what a lot of famous scientists looked like. Statues or portraits of people from hundreds of years ago were generally pretty poor quality and very fuzzy. Even after photography arrived there were often not very many good pictures.
Now with generative, AI you can fill in the missing images.
If you do a Google image search for Charles Darwin, you will get a lot of grainy images of a very old man with a very large bushy beard.
To put him in a more meaningful context, I used the Leonardo.AI image generator with the following prompt: “Charles Darwin on the HMS Beagle”. I wondered if the question might be taken literally and I would get a portrait of a man riding on a dog. But the AI was smart enough to understand that the Beagle was a ship. This produced a vastly more satisfying portrait.

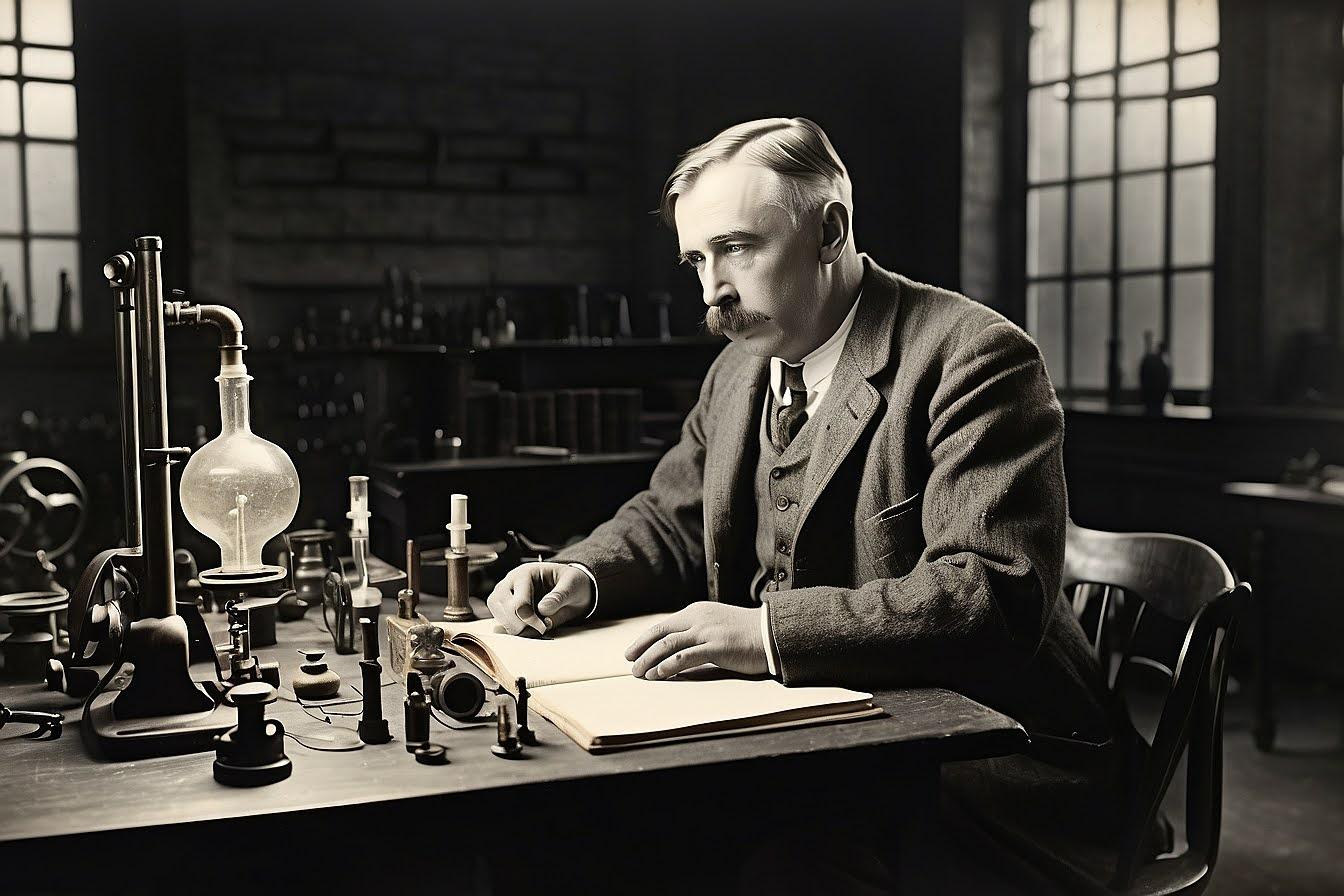
Next I was interested in a picture of Albert Einstein. There are many pictures of him but they tend to be of an older man with wild hair. So I asked for a drawing of “A young Albert Einstein”. Here’s what I got.

Not quite what I expected. It looked like an Einstein baby face with the wild gray hair of his older pictures. So I modified the request and asked for “A young Albert Einstein working in the patent office”.

I couldn’t quite make out what all those strange instruments on the desk were but it did look like a photo from 1902.
Next I decided to step back in history and try something a little more challenging. Euclid was a giant in mathematics. His axiomatic and deductive analysis of geometry established a fundamental logical basis for mathematical reasoning. There seems to have been only a few stylistic drawings of Euclid from the Middle Ages; not very interesting or revealing. So I asked the AI to do a picture of “Euclid teaching students in the Parthenon”. Here is the result which is what I imagine Euclid might have looked like in a historical context.

Another famous Greek scientist who was a mathematician, physicist, engineer, astronomer and inventor, was Archimedes. There’s a famous story of the king who gave him a crown that had been made for him but he wanted to know if the goldsmith had cheated him by substituting some cheaper silver for some of the gold. Archimedes knew that if he could calculate the volume of the crown, he could compare the weight of the crown to the weight an equal volume of gold on a scale. If the crown was lighter it would prove that a cheaper metal had been substituted for some of the gold.
While taking a bath Archimedes realized that the water in the tub rose by an amount equal to the volume of his body. He could submerged the crown in a bucket of water and the amount that the water rose would be the volume of the crown. Archimedes was so excited by this discovery, which came to be called Archimedes Principle, that he jumped out of the bath and ran naked through the street shouting “Eureka”.
Here’s the first drawing I got from the AI when I asked for this image.

I didn’t think that looked like a very good picture of Archimedes at all, so I asked the AI to generate some more images. With generative AI tools, you typically get several images for each request. With Leonardo.AI I generally got four images at the same time and they could all be quite different. In addition, you can ask it to repeat your request and you will get a different result, not the same thing over and over.
However, I seemed to continually be getting this cartoon caricature. It struck me that perhaps the training data for the AI had included a lot of images from some cartoon version of Archimedes. So I modified my request and asked for “The real historical Greek Archimedes jumping out of the bath”. This produced this rather dramatic picture. I preume that the object that Archimedes is holding is supposed to be the crown. If so, the king must have had a rather strangely shaped head.

Most people know that Leonardo da Vinci was an artist who painted two of the most famous masterpieces in the world: the Mona Lisa and The Last Supper. I always admired Leonardo more as the ultimate “Renaissance Man”. Besides being an artist, he was also a scientist, philosopher, engineer, and mathematician.
Leonardo studied many things and his observations and drawings fill many notebooks, containing over 10,000 pages. Some of the things found in Leonardo’s work relate to geology, anatomy, the flight of birds, how water flows with designs for dams and canals, botany and various flying inventions such as a helicopter, a parachute and a hang glider.
Here is Leonardo AI’s image of Leonardo the Engineer working on one of his designs for a flying machine.

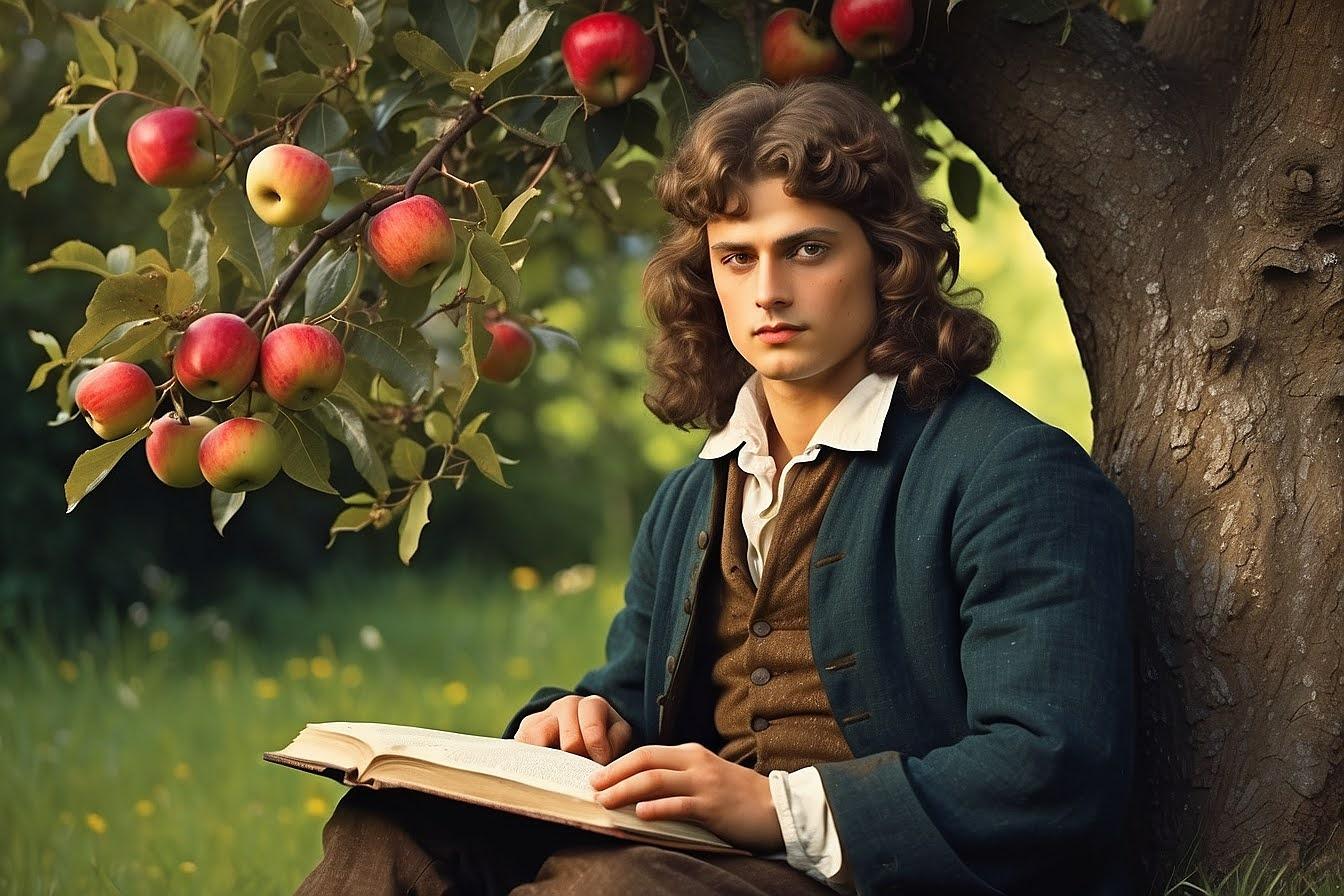
A gallery of famous scientists would not be complete without a picture of Isaac Newton.Most images of Newton on the Internet are formal portraits of a middle aged man with very long hair. Most people know the story of Newton’s discovery of gravity by watching an apple fall from a tree so to try and see Newton in the context of history, I asked for a picture of “a young Isaac Newton thinking under an apple tree”. I thought this result was quite lovely.
But among the several other images that the AI presented was the following. I guess the AI had used training data that had some pictures of a dog named Newton that had been posted on the Internet.

One of the greatest and most prolific mathematicians in history was Leonhard Euler (1707–1783) but he is unknown to many people. Some may know that the symbol e for the base of natural logarithms which occurs in many mathematical formulas is named for him. A few more may know about Euler’s Identity, named in a poll as the most beautiful theorem in mathematics.
eiπ + 1 = 0
Euler lived in Konigsberg, Prussia for a few years. The town had seven bridges that connected two islands and the other side of the river. It was a local challenge to see if anyone could go on a walk that would cross each bridge exactly once.
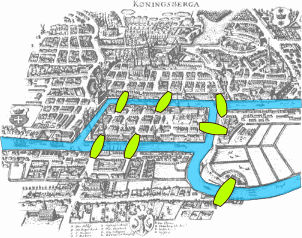
Euler proved that such a walk was impossible. While this may not have been one of the most important problems for a great mathematical mind like Euler, in fact it was significant. His solution involved abstracting the problem and it laid the foundation for graph theory and topology as mathematical disciplines.
The Seven Bridges of Königsberg
To present Euler in an interesting historical context, I asked the AI for a picture of “Leonhard Euler crossing the Konigsberg bridge”.

A famous name in the history of computers is Ada Lovelace (1815-1852). Her math tutor introduced her to Charles Babbage, a mathematician who was also active as an astronomer. He was building a mechanical calculator which incorporated many mechanisms that were similar to a modern computer. Ada was fascinated by this and worked with him on some of the programs that they were developing to calculate various mathematical tables. Babbage’s Difference Engine is considered to be one of the first computers and Ada Lovelace is considered to be one of the first computer programmers. Here is a generated picture of Ada Lovelace operating the Babbage Difference Engine.

If you’ve ever visited St John’s Newfoundland, you may have trekked up to Signal Hill to see the stunning views overlooking St John’s Harbor and the Atlantic Ocean. Signal Hill is a National Historic Site of Canada. There was a major battle between the French and English in 1762 but to my mind a more significant event that occurred there was the first transatlantic radio communication.
Guglielmo Marconi had been experimenting with “wireless telegraphy” since he was a young man. In 1994 he built a radio transmitter that could ring a bell on the other side of a room. A few years later he was successful in sending the first wireless communication over the open sea and in 1899 he transmitted a signal across the English Channel. Marconi then built a high powered station in Cornwall and prepared an experiment to transmit a signal across the Atlantic Ocean. Marconi traveled to Signal Hill to witness the reception. Here is a generated image of that historic moment.

However, if you look closely, there are two dignitaries standing by the radio receiver, and they both look like Guglielmo, as does a third man seated to the right. But there is no record that there were Marconi triplets. This is another case of how AI, still in its early days, makes mistakes.
No one should need an introduction to Marie Curie and her discovery of radioactivity. She was the first woman to win a Nobel Prize and the only person to win a Nobel Prize in two scientific fields (Physics 1903, Chemistry 1911). As such she was famous in her lifetime and there are many photographs of her. However I was able to generate this rather dramatic picture of her by asking for “Marie Curie discovering radioactivity in her lab.”

Another scientist investigating radioactivity was Ernest Rutherford. He discovered the element radon and alpha and beta radiation, among many other things. He was the first one to “split the atom” which he did by bombarding nitrogen with alpha particles that triggered the emission of protons. Rutherford was awarded the Nobel prize in 1908 and came to be known as “the father of nuclear physics”. In spite of his many accomplishments, he is not that well known outside of the field. I added “Sir” Ernest Rutherford to my gallery, not because of a shared belief in “The Importance of Being Earnest”, a rather Wilde play deserving of an Oscar, but because I had a more fateful connection with him.
Rutherford was a professor at McGill for a few years around the turn of the century and he did a lot of experiments in radioactivity in his lab in the physics building. When I entered McGill, word had it that he had contaminated the building with his radiation experiments. That old building still existed and is where I went for my physics classes and labs. Working in a radioactive lab may have earned Sir Ernest a Nobel Prize, but I don’t think it did me any good.
In 1928 Margaret Mead published the book “Coming of Age in Samoa”. This work challenged prevailing notions about human development and emphasized the importance of cultural context. It launched Mead as a pioneering researcher and she became the most famous anthropologist in the world. Mead set new standards for anthropology fieldwork through her detailed observation methods and use of photography, film and psychological testing.
Here is the result of asking for a picture of Margaret Mead in Samoa. This is very realistic and looks like an actual photo. However I did a Google image search and there is nothing like this photo on the Internet.

Many people learned about Alan Turing from the Hollywood film “The Imitation Game” that was nominated for eight Academy Awards in 2004. However, Turing was not well known in his lifetime, because the story of breaking the German code Enigma in World War II was classified for many years after the war. The first public revelation came in 1974 but the role of Alan Turing and others at Bletchley Park did not become known until the 1980s and 1990s as more documents were declassified.
The general impression given in the movie and in the media is that to break the Enigma code Turing invented one of the first computers. This is not accurate because the machine he built, “the Bombe”, was not really a computer but more of a specialized electromechanical device that could rapidly test multiple possible settings of the Enigma machine. There was another team at Bletchley Park working on breaking a different German encryption code that did design and build a machine, the Colossus, that in fact was one of the first computers ever built.
Here’s an AI generated picture of “Alan Turing breaking the code on an Enigma cipher machine”.

Another scientist of the World War 2 era who was featured in a major Hollywood movie was J. Robert Oppenheimer. The film “Oppenheimer” received 13 Academy Awards nominations and won 7 Oscars in 2024.
Oppenheimer first started his graduate studies in Cambridge but he was not adept with the laboratory work. To complete his Phd he went to the University of Göttingen, one of the leading centers of theoretical physics. At the time Europe was the center of the new age of quantum physics whereas American physicists were more experimental. During his time in Europe, Oppenheimer met many of the leading theoretical physicists in the world. When he was later recruited for the Manhattan Project he became a wise choice to be the head of development at Los Alamos since he could recruit many of the top physicists in the world, such as Enrico Fermi, Hans Bethe, Niels Bohr, Leo Szilard, Edward Teller and Stanislaw Ulam.
During the war the development of an atomic bomb was top secret but after bombs were dropped on Hiroshima and Nagasaki, Oppenheimer became a well known public figure.
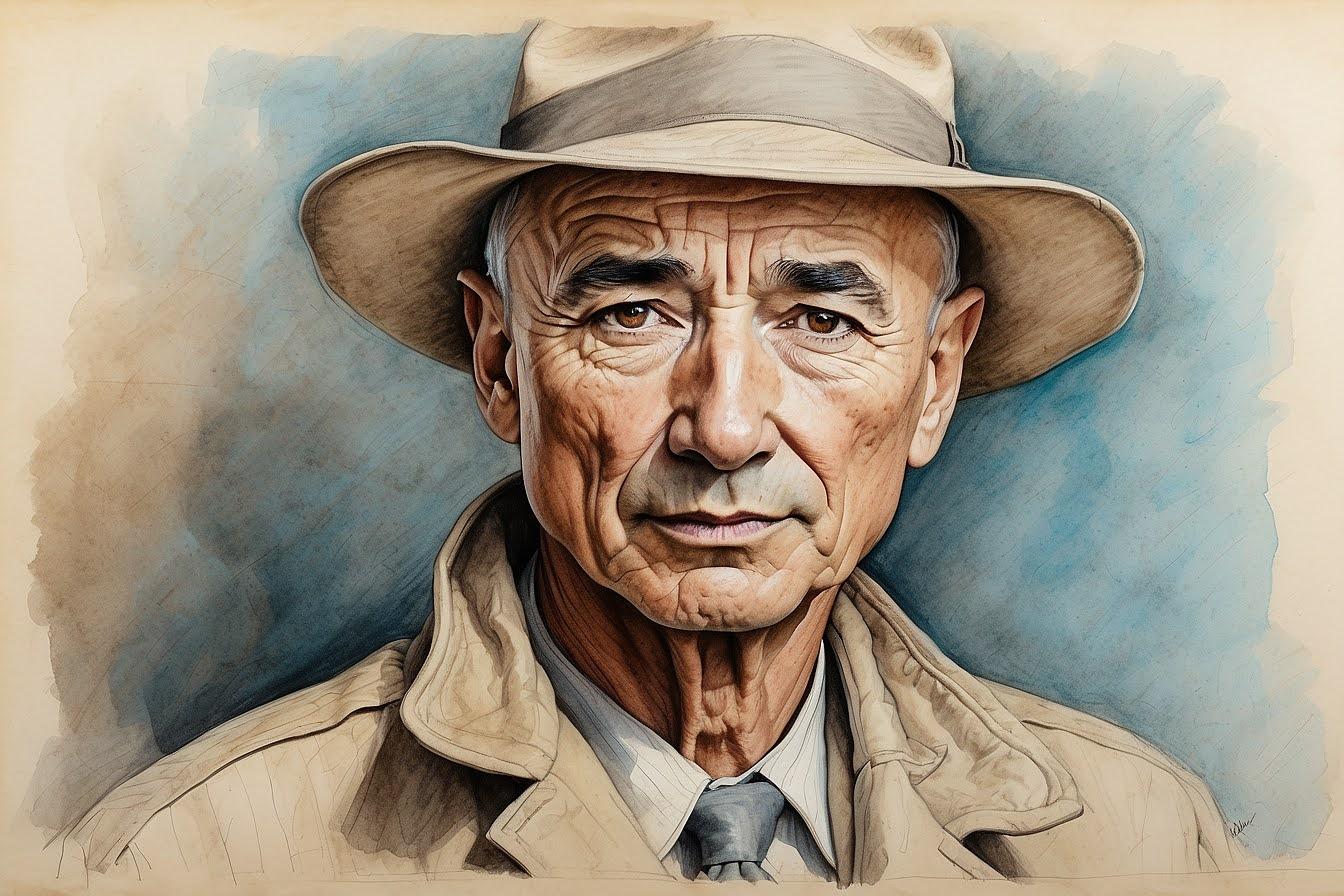
There were a lot of photographs of Oppenheimer so I asked for an AI generated sketch portrait instead of a photograph. Most image generators have a number of different styles that you can use, such as photographic, cinematic, concept art, graphic design and sketch drawings. Here’s the portrait of Oppenheimer which is quite good as a drawing and has a very good likeness to photos of him.
I also tried a few pictures of Oppenheimer at work. Here’s the result of asking for “Oppenheimer inspecting the nuclear test bomb Fat Man in the desert at Los Alamos.”

I have no idea how the AI went so far off the rails on this one. Maybe there were some training data images of garden statues that were called “Fat Man”. In the AI world, these sorts of wild errors have come to be called hallucinations.
Oppenheimer was a great movie in many regards in portraying many of the brilliant scientists who were working on one of the great scientific projects in history. However, there was one really glaring omission. The film never mentioned John von Neumann, one of the most brilliant minds of the 20th century. Von Neumann was the youngest person ever appointed to the Institute for Advanced Study at Princeton in 1933 at the age of 29, the same year that Albert Einstein was appointed, at age 54. Many of the top scientists who worked with von Neumann had stories or comments about his genius. Hans Bethe, one of the key physicists on the Manhattan Project, said “I have sometimes wondered whether a brain like von Neumann’s does not indicate a species superior to that of man”.
Von Neumann was not part of the Los Alamos team. When the bomb design ran into a critical problem, Oppenheimer contacted von Neumann to become a consultant to the Manhattan Project. Johnny had been the first to establish a rigorous mathematical framework for quantum mechanics. He developed a mathematical model of the atomic reactions and worked with the physicists at Loa Alamos to design an implosion that would trigger the chain reaction that would produce an atomic bomb.
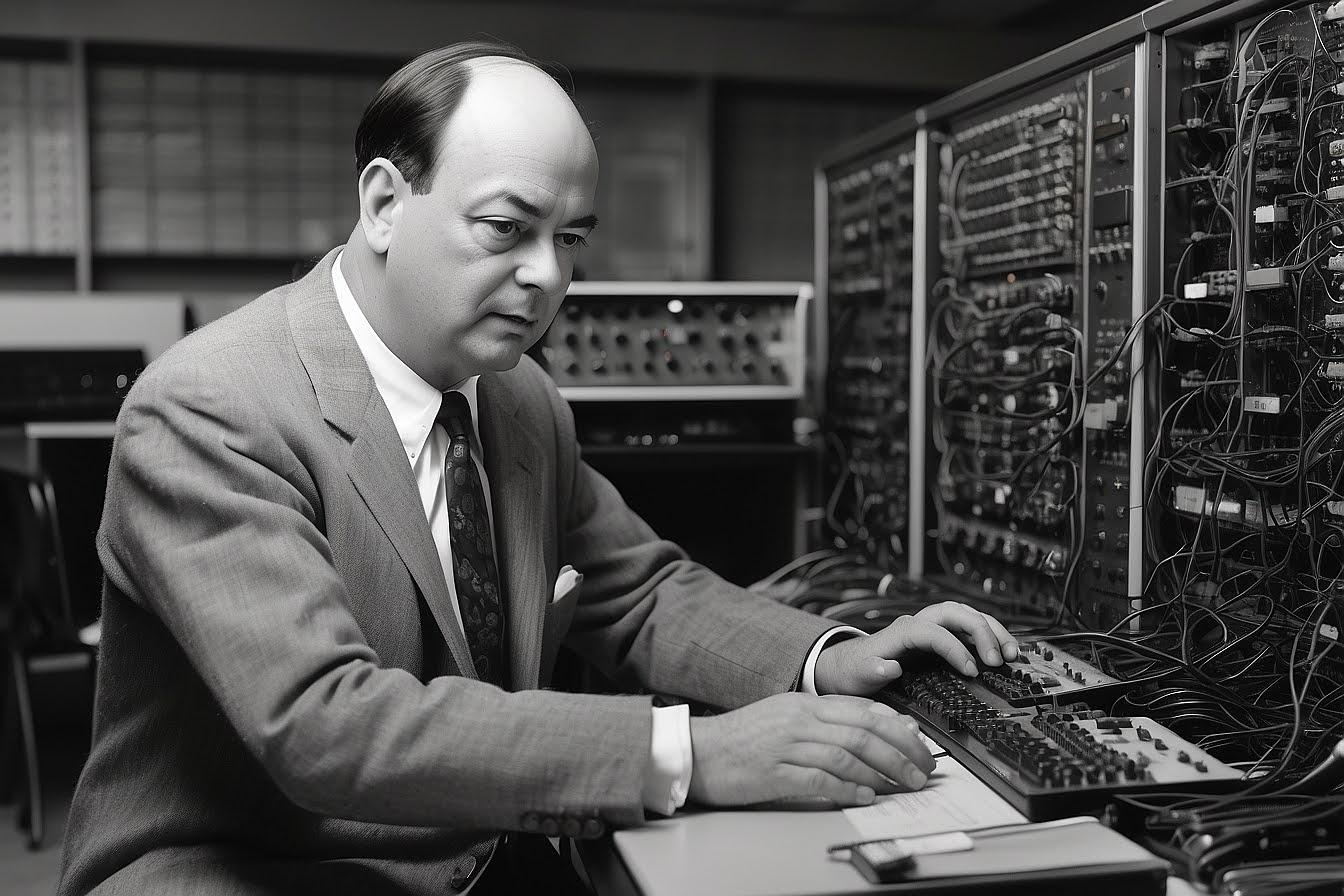
On one of von Neumann’s long train trips to Los Alamos, he wrote a paper describing the design for a computer. One of his revolutionary ideas was to use memory to store the program. This allowed the computer to be reprogrammed for different tasks without rewiring the physical hardware. This stored-program design came to be known as the von Neumann architecture.
Von Neumann began a project at the Institute of Advanced Studies to build such a computer. He published progress reports and many other projects around the world used this information to design and build their own computers, notably IBM’s first computer, the IBM 701 that was released in 1952. Since then, almost all computers, from mainframes to micro computers to mobile phones are fundamentally von Neumann architecture machines.
Here’s the AI generated picture of John Von Neumann programming the IAS computer at Princeton.
Overall, I would give image generation AI a score of maybe 7/10. Some of the results are quite stunning, dramatic and accurate. On the other hand, there are many that miss the mark and occasionally go off the rails.
It’s clear to see that in spite of the hype about AI and worries about it taking over jobs and controlling the world, AI has a long way to go and is not ready for prime time. Except for some cases, like Newton the dog, Einstein the baby and Fat Man the garden statue, which are ready for prime time, on the comedy channel.